Coronavirus Is an Occupational Disease That Spreads at Work
For both Democratic and Republican politicians, blaming social gatherings for coronavirus’s spread is convenient. But they’ve ignored or denied the central role workplace transmission plays in driving up infections. We need to treat coronavirus as the occupational disease it is — and that means restricting the power of business owners.

Employees of the New York MTA carry out overnight subway disinfecting and cleaning, and homeless services outreach during the early months of the coronavirus pandemic. (Marc A. Hermann / Flickr)
What is the one setting that accounts for most coronavirus transmission in the United States? Many governors believe they have the answer to this question. In countless press conferences and public statements, they claim that transmission primarily happens at social gatherings with friends and family.
The risk is particularly high, according to these political leaders, when the meetings do not happen in spaces that generate profit or serve important institutional functions. In contrast, US politicians have largely ignored, and even outright denied, the central role that workplace transmission plays in driving up coronavirus rates across the country.
Blaming social gatherings is politically convenient — it requires no restrictions on the power of business owners. In contrast, acknowledging that the coronavirus is an occupational disease highlights the need for public health interventions that are expensive to those in power.
Capitalism and Contagion
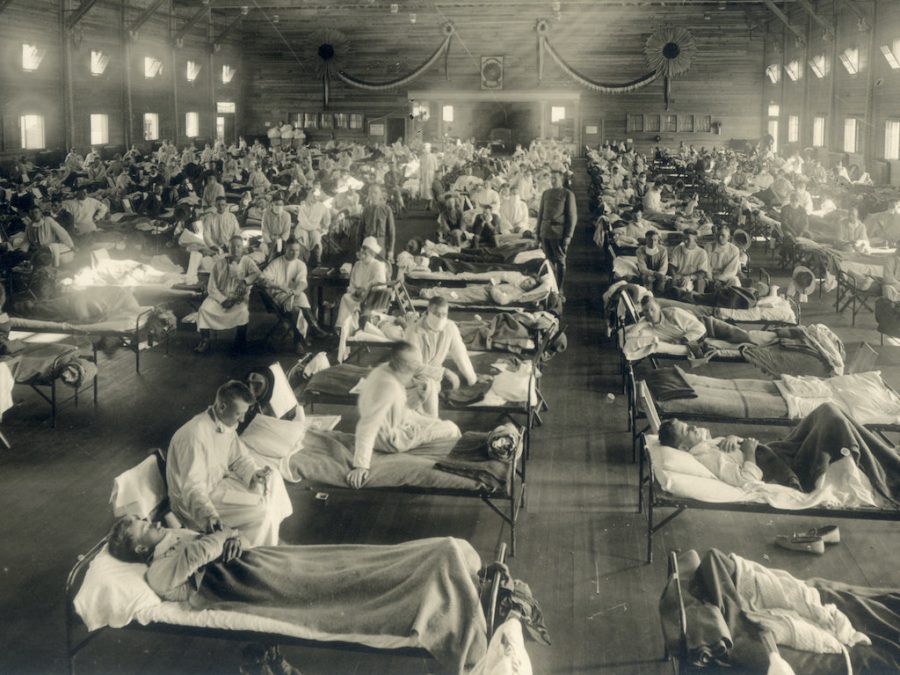
Business interests have shaped explanations of disease transmission throughout the history of capitalism. The medieval practice of quarantine fell out of favor among European powers in the first half of the nineteenth century. England and Holland loosened their quarantine laws in 1825, France in 1828, and Austria in 1841. Prominent physicians argued that restricting travel and detaining ships did little to control cholera, yellow fever, and the other epidemics that plagued Europe.
In heated public debates, these scientists contended that most diseases did not spread through contagion, inanimate poisons transmitted via close contact with an ill traveler, but rather through miasma, the noxious airs emanating from urban slums’ filth. According to noted anti-contagionists like Edwin Chadwick, author of England’s notorious Poor Laws, it was sanitation, not quarantine, that would keep disease away.
But the contagion vs. miasma debate also had an economic dimension. Quarantine was expensive. Enforcing quarantines slowed trade and relied on a powerful regulatory state, which conflicted with the goals of a newly empowered capitalist class. In light of these economic and political considerations, the downfall of quarantine seemed all but predetermined.
Science has advanced at such a pace that it would be hardly recognizable to a nineteenth century anti-contagionist. Virologists in China sequenced the genome of a novel coronavirus and shared it with the world just one month after the first outbreak in Wuhan. It was downloaded by US scientists, who then created the backbone of an effective vaccine in a mere two days, though it would take most of the next year to test.
Researchers also reached a consensus that respiratory droplets, carried through the air, were responsible for most coronavirus transmission. This last fact poses a major inconvenience to humans who like and often need to be physically close to one another.
Despite the rapid pace of biomedical science, the question of how the coronavirus moves through populations — which settings and activities contribute most to its overall spread — remains obscured in a miasmatic haze. In the United States, most coronavirus infections are never confirmed by testing, and most positive tests are never traced to a probable source. Detailed outbreak investigations that reach definitive conclusions are exceedingly rare.
Mapping the dynamics of viral spread requires the sort of strong public health infrastructure that does not exist in the United States. Even countries that have invested more resources into disease surveillance cannot keep up when infection is widespread, as there are too many potential sources of infection. Perhaps most importantly, properly investigating the question of where the coronavirus spreads also requires those in power to want to know the answer.
Governors Don’t Want to Hear It
Amid this uncertainty, governors across the country attributed the pandemic to social gatherings while downplaying the role of other settings. Arizona governor Doug Ducey, for instance, told the press, “Most of the spread we’re seeing cannot be traced to restaurants or small businesses . . . Most of this traces to small gatherings of family and friends like the Thanksgiving holiday which was just two weeks ago.”
Rhode Island governor Gina Raimondo echoed this message, “We know that spread is happening in these casual, social settings,” she wrote in a statement. In contrast, Raimondo contended that spread was “not happening in larger but more structured environments” such as offices, buses, and schools.
In Massachusetts, Governor Charlie Baker decided to ease restrictions on businesses, explaining, “Many of our clusters have been the result of informal gatherings.” Baker continued: “Work, in many cases, is not where spread develops because people at work are relying on and abiding by the rules and the guidance.”
But there may be no stronger proponent of the social gathering hypothesis than Andrew Cuomo. In a November press conference, the New York governor laid the blame for viral spread solely on personal irresponsibility.

“If you’re socially distant, and you wore a mask, and you were smart, none of this would be a problem. It’s all self-imposed.” He continued, “If you didn’t eat the cheesecake, you wouldn’t have a weight problem.”
Cuomo later inaugurated an ad campaign warning New Yorkers against holding social gatherings in their homes. Its central claim — that over 70 percent of coronavirus transmission can be attributed to “living room spread” — was based on an unusual analysis of contact tracing data.
As would be expected, the 70 percent figure counted transmission between friends who decide to meet up for a birthday party (a social gathering), but it also included infections between family members who live together (within-household transmission). Data from other states suggests that within-household transmission likely accounts for nearly all “living room spread,” and one must also wonder how the virus entered the home in the first place.
To be sure, social gatherings likely do play an important role in coronavirus transmission. Research has shown, for instance, that national bans on social gatherings are one of the most effective interventions to limit viral spread. Social gatherings may also explain why, in some places, transmission increases after major holidays.
But there are many important observations that the social gathering hypothesis cannot explain. Chief among them is the extreme racial inequality in infection rates. White people in the United States appear to be the most likely to attend social gatherings during the pandemic, but are among the least likely to contract the coronavirus.
As much as social gatherings have dominated American public health messaging, the role of infection in the workplace has been largely ignored. The main exceptions occurred early on in the first wave of the pandemic. First, a shortage of masks and other personal protective equipment dominated a few news cycles as physicians and nurses treating coronavirus patients protested unsafe conditions. While shortages have not been fully resolved, the issue no longer garners much public attention.

Second, large outbreaks in meatpacking plants — where thousands of workers toil in close quarters — raised the specter of a national food shortage. President Trump invoked the Defense Production Act in late April to force meatpacking facilities to remain open, even as the plants had been identified as super-spreading sites that potentially drive up virus rates in surrounding communities.
The plight of meat processing workers has also largely receded from national attention, with the exception of a widely publicized lawsuit in November: managers in an Iowa pork facility placed cash bets on the number of workers would contract the virus, the plaintiffs allege.
While meatpacking plants are unique in their size and centrality to food distribution, comparably crowded, poorly ventilated conditions can also be found in factories, restaurant kitchens, warehouses, and construction sites. There is an added risk of interacting with many customers for those who work as cashiers, hairdressers, home care providers, and food servers. Despite this, health department data on coronavirus transmission in workplaces tends to be thin and unreliable.
A restaurant owner in Little Rock, Arkansas was dismayed when the state never investigated an outbreak among ten of the restaurant’s workers and never included the incident — or any other restaurant outbreak — in its public reports of disease clusters. “I think there’s probably a lot more clusters in restaurants than anybody really wants to admit,” she lamented.
Even the few states that collect data on the occupation of coronavirus patients do so poorly. Massachusetts, for instance, legally requires reporting of employment categories, but, in practice, the data is missing for 84 percent of positive tests.
It Spreads at Work
Scant as it is, the research on workplace exposure paints a picture of the coronavirus as a concerning occupational illness that contributes substantially to community spread. A study of a large grocery store in the Boston area found that employees with customer-facing jobs were about five times more likely to have coronavirus antibodies than workers in other roles.
Additional studies have attributed high rates of infection to workplace exposures in agriculture and construction. In a survey of service workers, 41 percent responded that they were not able to consistently maintain physical distance from others on the job.
Workplace exposure also offers a compelling explanation for much of the racial inequality that has characterized the pandemic. Black, Latino, and indigenous people are not only more likely to die of coronavirus than white people, but all evidence indicates that they are also more likely to be exposed and infected.
People of color make up a large share of essential workers in high-risk industries and are more often linked to workplace transmission than white employees. Mobility data from cell phones shows that, during the pandemic, the only difference in travel patterns between residents of wealthy neighborhoods (who tend to be white) and residents of low-income neighborhoods (where many people of color live) is that residents of low-income neighborhoods spend a lot more time at work.
The pandemic’s uniquely devastating toll on Latino communities also points to the centrality of workplace exposure. Latino workers are concentrated in some of the highest-risk industries such as food processing, food service, construction, and farm work. In a normal year, the overall mortality rate for Latinos is lower than that of white people. It therefore was not obvious that the virus would kill Latinos at uniquely high rates.
But between January and October 2020, Latinos experienced the highest excess mortality of any racial group, dying at 50 percent above their normal rate compared to an increase of just 10 percent for white people and about 30 percent for other races. The mortality rate increase has been particularly striking for working-age Latino men.

While avoiding social gatherings is largely a question of personal choice, avoiding workplace exposure requires a shift in the balance of economic power. Workers in the United States are not well-positioned to protect themselves from occupational exposure to the coronavirus, but they are putting up a fight. Workers throughout the country have organized strikes and other labor actions since the start of the pandemic.
Many of these have involved demands for stronger coronavirus protection measures. However, the success of these protests has been limited to a small number of workplaces and, as Mike Davis laments, the United States has not yet seen a national protest movement to demand a stronger pandemic response.
Alongside organizing efforts, thousands of workers have also made phone calls to the Occupational Safety and Health Administration (OSHA), particularly as the first wave of infections crested. The calls largely went unresolved, however. In pre-pandemic times, OSHA operated as an underfunded regulatory agency with limited enforcement powers. Under the leadership of Labor Secretary Eugene Scalia, OSHA has been particularly hamstrung by the administration’s refusal to issue a regulation that would specifically protect against coronavirus exposure.
Still in the Thick of It
The Food and Drug Administration’s emergency authorization of two vaccines seems to offer a way out of the crisis of workplace coronavirus infection. A Center for Disease Control advisory panel recommended prioritizing all twenty-one million health care workers for vaccination (along with nursing home residents) in the first phase, and thirty million other high-risk “frontline” workers (alongside all Americans older than seventy-five) in the second phrase.
But the vaccination process has rolled out slowly due to limits on production and inefficient distribution. Many health care workers employed through staffing agencies or independent contracting arrangements have found themselves entirely excluded from vaccination plans.
A number of states including Florida and Texas have declined to include frontline workers as a vaccination priority category. Even states that have prioritized frontline workers do not have well-designed distribution plans, and it is not clear if they will set up clinics at worksites to reach those most in need.
The governor of Nebraska went as far as to state that undocumented immigrants — many of whom work in the state’s meatpacking plants — will be excluded from the frontline worker priority group. Perhaps most crucially, the ability of the vaccines to prevent asymptomatic spread from workers to still-unvaccinated friends and family remains an open question. Even in the most optimistic scenario, without quickly enacted public health interventions, the United States is facing a devastating toll of further deaths before vaccination becomes widespread.

There is one set of public health interventions that governors can implement quickly enough to prevent a far higher death toll: pay millions of workers to stay home while temporarily closing and restricting businesses, universities, and other institutions. This is the course of action favored by most Americans, who support closures of nonessential businesses by a two-to-one margin. Many cities and states closed businesses in the spring of 2020, which successfully drove down viral transmission.
While the economic restrictions created widespread unemployment, a large majority of newly laid off workers actually earned more with the weekly $600 unemployment insurance supplement — paid for through federal CARES Act funding — than they had on the job. Combined with lump sum stimulus payments, the net effect of the economic interventions was to temporarily lower the US poverty rate to below pre-pandemic levels while allowing people to avoid workplace exposure.
When workplaces reopened, some workers rejected the opportunity to work under hazardous conditions for little pay. But business owners could prevent non-returning workers from receiving benefits by reporting them to the state unemployment office. In an act of defiance, one anonymous hacktivist flooded the Ohio state unemployment website with thousands of fake reports to render it inoperable.
By late fall 2020, when coronavirus rates were ticking up across the United States, the $2.2 trillion in CARES Act funding had long since dried up. Congress made additional funding available in late December but — at a paltry $900 billion, with an unemployment supplement only half as large as the spring’s — it was not fully up to the challenge of buffering the blows of further economic restrictions.
As the death toll rises over the winter, mayors and governors are reluctant to impose further economic interventions. In early January, only four US states have fully banned indoor dining at restaurants, and many gyms, salons, and retail shops remain open.
Andrew Cuomo succinctly articulated the widespread opposition to economic interventions on the part of political leaders, “The cost is too high,” he said, and by the time the pandemic eases, “we will have nothing left to open.”
As with nineteenth-century quarantine, economic interventions that protect workers from coronavirus exposure are expensive and require a strong regulatory state. But unlike the anti-contagionists of two hundred years ago — and unlike American governors in 2021 — almost no prominent scientists vocally oppose economic restrictions or deny their effectiveness.
Still, in their public statements, American scientists have ignored the issue of economic interventions altogether and have instead echoed the messages of state and local leaders, urging individuals to change their behavior by wearing masks, avoiding social gatherings, and receiving the vaccine when available. Rather than trying to shape the contours of the pandemic response, scientists largely content themselves with the well-worn fantasy that they operate within a narrow and predetermined range of political possibility.
This has resulted in a missed opportunity, particularly in light of imminent Democratic control of the presidency and both chambers of Congress. A multi-trillion-dollar funding package that would encourage and enable states to shut businesses and institutions is not even on the political radar because — unlike their counterparts in the United Kingdom and Canada — American scientists have not identified it as a desirable goal.
With no clear guidance about what to fight for, progressives have demanded larger stimulus checks and student loan forgiveness which, while providing economic relief to many in need, would do little to impede the ever-rising toll of illness and death.
In the end, however, the reason American political leaders have allowed the coronavirus to spread nearly unabated comes down to the question of who is harmed and who has power. During the first year of the pandemic, US billionaires amassed an additional $4 trillion of wealth. But it was not just the few at the very top who were better off: the combined net worth of US households is the highest in the nation’s history, buoyed by strong performance in the stock and real estate markets.
Amid mile-long food pantry lines, employment rates for the top-paying third of jobs have fully recovered. Furthermore, the same populations that remain economically unscathed have also been insulated from the worst effects of the coronavirus on their health — they are least likely to be infected or die from the disease.
If American political leaders continue on the same course, hundreds of thousands more people will die preventable deaths before the pandemic subsides. The worst effects of the virus will continue to be concentrated among workers and their older family members.
Though he was describing the industrial slums of Manchester in the nineteenth century, Friedrich Engels coined a term that well-describes the actions of the US ruling class today: social murder.